
Title
Ebola virus Glycoprotein with Increased Infectivity Dominated the 2013-2016 Epidemic
Journal
Cell 167(4):1088-1098 (2016)
Authors
Diehl WE, Lin AE, Grubaugh ND, Carvalho LM, Kim K, Kyawe PP, McCauley SM, Donnard E, Kucukural A, McDonel P, Schaffner SF, Garber M, Rambaut A, Andersen KG, Sabeti PC, Luban J
Abstract
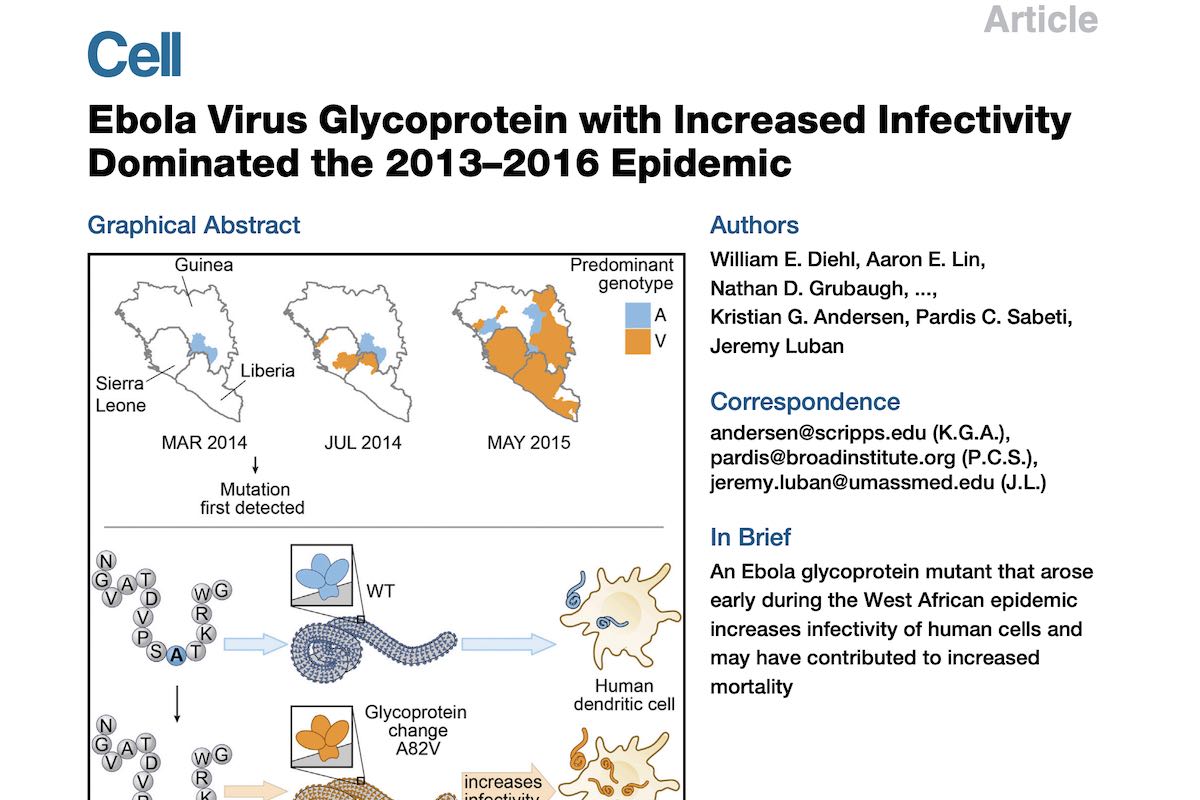
The magnitude of the 2013-2016 Ebola virus disease (EVD) epidemic enabled an unprecedented number of viral mutations to occur over successive human-to-human transmission events, increasing the probability that adaptation to the human host occurred during the outbreak. We investigated one nonsynonymous mutation, Ebola virus (EBOV) glycoprotein (GP) mutant A82V, for its effect on viral infectivity. This mutation, located at the NPC1-binding site on EBOV GP, occurred early in the 2013-2016 outbreak and rose to high frequency. We found that GP-A82V had heightened ability to infect primate cells, including human dendritic cells. The increased infectivity was restricted to cells that have primate-specific NPC1 sequences at the EBOV interface, suggesting that this mutation was indeed an adaptation to the human host. GP-A82V was associated with increased mortality, consistent with the hypothesis that the heightened intrinsic infectivity of GP-A82V contributed to disease severity during the EVD epidemic.
Additional Background
In a recent study published in Cell together with colleagues from UMass Worcester and the Broad, we show how a single mutation that occurred during the 2013-2016 Ebola virus disease epidemic in West Africa increased the ability of the virus to infect human cells. The mutation occurred in the Ebola virus glycoprotein and is located in the receptor binding domain of the protein. This is the first ‘natural’ mutation in the receptor domain of the virus – prior to this epidemic, this part of the virus had always been fully conserved. In a series of experiments, we show how this single mutation – GP-A82V – led to an increased ability of the virus to infect primate cells, but not other mammalian cells. A separate study published back-to-back also showed that this mutation decreased the ability of the virus to infect bat cells – bats being the presumed reservoir of Ebola virus. These studies provide evidence to suggest that the GP-A82V is a human adaptive mutation and a separate study in Journal of Virology adds to this picture by showing that viruses carrying the derived (GP82V) allele have a fitness benefit over the ancestral (GP82A) form.
The papers received a lot of news coverage, unfortunately (but not unsurprisingly) leading to several wrong and hyped conclusions, the most common being:
- Ebola virus mutated to become more pathogenic/deadly/lethal during the outbreak
- A mutant form of Ebola virus was responsible for the size of the 2013-2016 outbreak
- Ebola virus evolved to become more transmissible during the 2013-2016 outbreak
All of these claims are false – none of the studies show any of this. What they DO show, is that the mutation caused the virus to become better at infecting human cells. This makes sense, and because of the jump from bats to humans, is very much within the realm of what we would expect. This increased ability to infected cells, however, does not (necessarily) translate to an increased ability to infect humans, transmit better, or cause more severe disease. In fact, it is highly plausible that such a mutation – while increasing the intra-host fitness of the virus – could lead to decreased between-host (transmission) fitness. It didn’t have to ‘compete’ with the ancestral form outside the host, so the reason why the derived GP82V form of the virus rose to such high prevalence could be entirely due to (well established) founder effects.
Let me give an example of this, based on when and how we believe the mutation occurred. Imagine that in a single patient (let’s call him ‘Patient X’) in Guinea, the Ebola virus GP mutation arose within this infected individual. This person would now have two forms of the virus – GP82A and GP82V. Initially, the derived (GP82V) version would be at a lower frequency than the ancestral (GP82A) form. However, since GP82V is more ‘fit’ within a host, it would quickly outcompete GP82A within Patient X. The study in Journal of Virology shows nicely such a ‘competition’ experiments.
Now imagine that this patient traveled to Sierra Leone (maybe for treatment) and transmitted the virus to several other people. Because GP82V would now have ‘won’ over GP82A in Patient X and be the predominant virus in this patient, it would be the one most likely to transmit to the next infected individual. The derived GP82V form of the virus now found itself in a new country – Sierra Leone – that up until this point had not reported any cases. The GP82V virus was now free to roam and all subsequent transmission from this single event in Sierra Leone would mean that everybody would end up being infected with GP82V – not GP82A (the ancestral virus) since GP82A wasn’t in Sierra Leone. Other factors – community resistance, broken healthcare, no contact tracing, etc. – could then lead to an explosive increase in cases in Sierra Leone. This would have nothing to do with whether the virus would have been GP82V or GP82A – this increase would have happened anyway. It also wouldn’t have depended on whether the virus was more or less fit within a single patient – since this tells us nothing about the virus’ ability to transmit. While I cannot prove that this is what happened – and many will disagree with me – I think this is a much more likely scenario than the virus having an increased ability to transmit. The importance here being that the selection pressure within host to increase fitness (e.g., increased ability to infect cells) happens on a faster timescale and is (likely) disconnected from the selection pressure for transmission potential. The former is almost bound to happen given the size of the outbreak, whereas the latter is unlikely over the observed time period.
Finally – and most importantly – once proven and effective Ebola prevention measures were put in place (primarily patient isolation + contact tracing) at the height of the outbreak, the number of cases started plummeting immediately and dramatically. This drop in case numbers was even more pronounced in countries where GP82V was highly prevalent (Sierra Leone and Liberia) compared to Guinea, where GP82A was still circulating. This single observation strongly suggests to me that there was nothing unusual about the transmission potential of GP82V – ‘standard’ Ebola measures were enough to prevent it from spreading further.
Ed Yong was the only one to get all of these caveats right and wrote what I consider a nicely balanced and non-hyped background article on the two stories. Trevor Bedford and Harmit Malik also wrote a very good commentary for Cell explaining many of details. I highly recommend you read both.
Media Coverage – the ones to read
Commentary in Cell – Did a Single Amino Acid Change Make Ebola Virus More Virulent?
Article by Ed Yong in the Atlantic – How Ebola Adapted to Us
Other Media
Scripps Research Press Release
Science
Time
New York Times
The Washington Post
Los Angeles Times
NPR
Fox News
BBC News
NBC News
New Scientist
Scientific American